|
| This is an educational web site by Dr. Dale Dubin (Dale Dubin, M.D.), which includes important EKG (ECG) information about EKG tracings, 12 lead EKG's, and cardiac monitors. All web sites offer free PDF downloads.
To order Rapid Interpretation of EKG's, scroll to the bottom of the page. |
|
Midway
through the last century, a unique learning tool emerged, facilitating
the comprehension of difficult subject matter. This technique
known as "programmed instruction" became a popular method for
learning complex disciplines. Contrary to popular belief, Dr.
Dubin did not invent programmed instruction.
According
to an anecdotal story, a mathematician's daughter was having difficulty
grasping the principles of college calculus. Every day the mathematician
would compose and mail a simplified concept of only a few sentences,
along with a brief diagram to his daughter. The calculus principle
of a given day was linked theoretically to that of the previous
day and designed to lead into that of the following day. By reading
her daily measure of concatenated logic, the daughter soon became
a calculus whiz.... so the story goes.
In
order to strengthen comprehension, the body of the text is reduced
to single sentences that approach each new concept from various
aspects. In this way, small doses of didactic medicine bring the
concept into focus. Once the concept(s) of one page are mastered
(reviewing the diagram as needed), the reader proceeds to the
next page, which is carefully concatenated (linked) to the conceptual
material on the following page.
The
illustrations in Rapid Interpretation of EKG's use real
EKG tracings (not simulations), so what you see, is what you will
experience professionally. Students in the medical sciences, often
intimidated by electrocardiography, welcome this learning-by-understanding
method. Memorizing patterns of EKG's has a dismal half-life. Using knowledge anchored in understanding, readers
are pleased that, in a subtle manner, they also learn about cardiac
physiology, pathology of the heart, and care of patients. The
tradition persists.
The
most popular programmed texts owe their success to reader/student
feedback. No author has been able to anticipate pages that might
be difficult for neophytes to comprehend. So, reader input has
become instrumental in the evolution of such texts. New explanatory
text is added with each new printing to ease the learning process
through areas of intellectual turbulence. The author guides your
progress for rapid, seamless comprehension.
Through
the years, contemporary "programmed instruction" has
evolved into "interactive learning" whereby the reader
actively participates in his own learning process. Medical education
need not be an oppressively serious task. Through the years Dr.
Dubin's sense of humor has been persistently woven into the dialog
with the reader, lightening the tensions of study. Many authors
have mimicked his friendly, easy-going style.
This
section should be downloaded by now, but if it is not quite ready,
please be patient a little longer. At the end of this section
you will be amazed at how much practical information you have
absorbed.
|
Rapid Interpretation of EKG's employs interactive learning to achieve
maximum understanding.

The
color illustrations from the new 6th edition are designed to display familiar
(often entertaining) images for visual association and instant recall.
This is a very effective, permanent memory tool.
|
From
Rapid Interpretation of EKG's copyright © 2017 COVER
Publishing Co. Inc.
Digitalis causes a gradual down-sloping of the ST segment, to give
it the appearance of Salvador Dali's mustache.
|
As you see in the above illustration, each page begins with a large, simplified
graphic representation that is explained by its caption. Link the following
sequence of illustrations in your mind.
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
Our main objective is to rapidly determine the heart rate from
the EKG.
|
| |
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
First: Find a specific R wave that peaks on a
heavy black line (our "start" line).
|
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
Next:
Count off "300, 150, 100" for every thick line that follows the
start line, naming each line as shown. Know these numbers; you will
use them throughout your career.
|
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
Then: Count off the next three lines after "300, 150, 100" as "75,
60, 50."
|
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
Now: Know these triplets so they are second nature. Make certain
that you can say the triplets without using the picture.
|
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
Where the next R wave falls, determines the rate.
It's that simple!
|
Wait a minute! If you consumed the illustrations and captions on the last
few pages, you can already determine cardiac rate on EKG. What an accomplishment
in such a brief time!
Once the image and the caption are understood as a unified concept, the
reader is encouraged to proceed with the simplified text below the illustration
(usually about three sentences). Notice how a missing key word encourages
interactive learning.
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
Myocardial infarction ("infarct") occurs when
a coronary artery supplying the left ventricle becomes occluded by a thrombus (blood clot),
so an area of the heart is without a blood supply.
The terms "myocardial  ,"
"coronary occlusion," and "heart attack" refer to the same
serious problem. ,"
"coronary occlusion," and "heart attack" refer to the same
serious problem.
The heart derives its own blood supply from the
arteries, so when a coronary artery or one of its major branches
is occluded, an area of the myocardium is without blood supply.
The infarcted area is primarily in the
ventricle, and deadly arrhythmias may result.
NOTE: We understand that the coronary arteries also supply the right
ventricle, so there is often some involvement of the right ventricle.
But since most of the critical problems originate in left ventricular
infarcts, myocardial infarction is usually conceptualized in terms
of the left ventricle.
|
The
illustration and caption fuse as a concept. Then the brief programmed
sentences below the illustration invite participation, in order to reinforce
your understanding of the concept. This is not an exam; in fact, returning
to an illustration for a word answer is a normal (planned) feature that
aids your comprehension.
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
Commonly, the thick left ventricle suffers myocardial
infarction.
The
left ventricle is the thickest chamber of the heart; so if the coronary
arteries are narrowed, the left ventricle (which uses the greatest
blood supply) is the first to suffer from an obstructed coronary
.
Blood
is pumped to all parts of the body by the powerful, thick,
ventricle.
NOTE:
When we describe infarcts by location, we are speaking of an area
of the left ventricle. Coronary arteries to the left ventricle usually
send smaller branches to other regions of the heart, so an infarction
of the left ventricle can include a small portion of another chamber.
|
The completed text sentences are designed for greater depth of understanding,
as they expand your grasp of each new concept with important related information.
Interactive learning is also designed to prepare your mind for the new
material ahead.
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
On EKG the QRS complex represents ventricular contraction. The Q
wave is the first downward wave of the QRS complex, and it is
followed by an upward R wave, however the Q wave is often absent
on EKG. Necrosis (death) of an area of the heart muscle produces
a Q wave on EKG.
The Q wave, when present, always occurs at the of
the QRS complex and is the first downward deflection of the complex.
The downward Q wave is followed by an upward
wave.
NOTE: If there is any upward deflection in a QRS complex that appears
before a "Q" wave, it is not a Q wave, for by convention, when
present, the Q wave is always the first wave in the complex.
|
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
The Q wave makes the diagnosis of infarction.
The diagnosis of myocardial infarction is usually based on the presence
of significant
waves that are produced by the area of necrosis.
NOTE: The Q wave is the first downward stroke of the QRS complex,
and it is never preceded by anything in the complex. In the QRS
complex, if there is any positive wave - even a tiny spike - before
the downward wave, the downward wave is an S wave (and the upward
wave preceding it is an R wave).
Significant Q
are absent in normal tracings.
We use a capital "Q" to designate a significant Q wave,
however small "q" waves are not significant.
|
This interactive method continuously reinforces what you have mastered,
while subtly relating important new facts that link to the concepts
ahead.
This interaction (with the author) facilitates learning and moves along
quickly. Quite effective, isn't it?
|
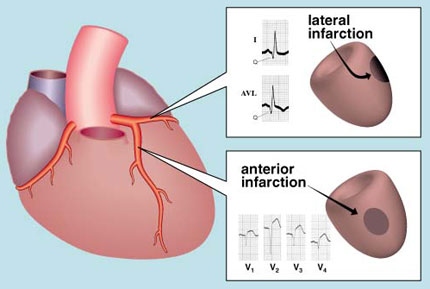
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
If there are Q waves in lead I and lead AVL, there is a lateral
infarction.
Please take a moment and glance at page 46 to make a mental note
of the leads that have a positive electrode located laterally on
the left arm.
A lateral infarction involves the lateral portion of the ventricle.
When a lateral infarction occurs,
waves appear in leads I and AVL.
NOTE: One might abbreviate Lateral Infarction as L.I. Just remember
AVL for "Lateral" and "I" for Infarction (after all, Roman Numeral
"I" for lead I is just a capital "i"). It's an easy way to recall
the leads that demonstrate lateral infarction.
|
Now
you can see why this type of programmed instruction has made Rapid
Interpretation of EKG's the world's best seller for over thirty
years!
|
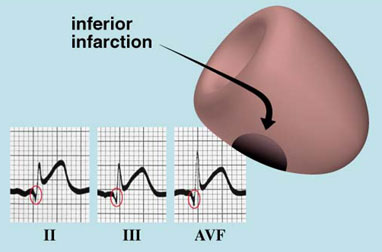
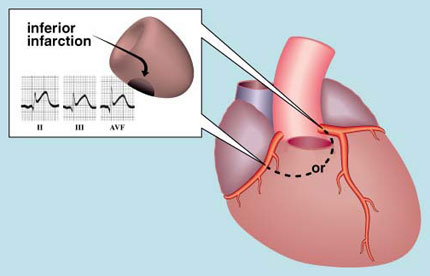
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
Inferior ("diaphragmatic")
infarction is diagnosed by the presence of Q waves in II, III,
and AVF.
The inferior wall of the heart rests upon the diaphragm, so the term
"diaphragmatic" infarction is sometimes used to indicate an infarction
in the inferior portion of the left .
An
infarction is identified by significant Q waves in leads II, III,
and AVF.
NOTE: If I told you the way that I remember the leads for inferior
infarction, this book would be banned. You may want to make your
own memory tool for remembering the leads for Inferior ("diaphragmatic")
Infarction using "two, three, and F."
|
An incorrect (missing word) answer is just as useful as the correct word
(perhaps better!), since it encourages reconsideration and rethinking
of the basic concept. This brief mental exercise reinforces a proper
understanding of the concept.
|
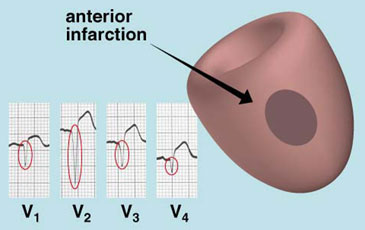
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
Q waves in chest leads V1, V2, V3, or V4 signify
an anterior infarction.
NOTE: The chest leads are mainly placed anteriorly on the
chest, so this is a good way to remember the leads for anterior
infarction.
The presence of Q waves in V1, V2, V3, or V4 indicates an infarction
in the anterior wall of the
ventricle.
NOTE: Statistically, anterior infarctions are very deadly, but fortunately,
immediate treatment with intravenous thrombolytic medications or
angioplasty with stenting has improved the survival rate substantially.
|
You're doing great! If you've been following the illustrations and text
so far, you know what a myocardial infarction is and how to make the diagnosis
on EKG. You also know how to identify the location of the main types of
infarction.
|
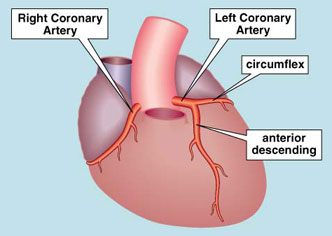
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
It is common practice to determine the general location
of an infarction, but with a little anatomical knowledge of the
heart's coronary blood supply*, we can make a far more sophisticated
diagnosis.
There are two coronary arteries that provide the heart with a continuous
supply of oxygenated .
Quickly review the illustration.
The Left Coronary Artery has two major branches; they are
the Circumflex branch and the
Descending branch.
The Right Coronary Artery curves around the right .
* The pulmonary artery has been "surgically" removed in this illustration
to show the origin of the coronary arteries at the base of the aorta.
|
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
A lateral infarction is caused by an occlusion
of the Circumflex branch of the Left Coronary Artery. An anterior
infarction is due to an occlusion of the Anterior Descending branch
of the Left Coronary Artery.
The Circumflex branch of the Left Coronary Artery distributes
blood to the
portion of the left ventricle.
The Anterior Descending branch of the Left Coronary Artery
supplies blood to the anterior portion of the
ventricle.
The Circumflex and the Anterior Descending are the two main
branches of the Coronary
Artery.
|
|
From Rapid Interpretation of EKG's copyright © 2017 COVER Publishing Co. Inc.
The base of the left ventricle receives its blood
supply from branches of either the Right or the Left Coronary Artery,
depending on which artery is "dominant."
Inferior ("diaphragmatic") infarctions are caused by an occluded
terminal branch of either the Right or the
Coronary Artery.
So the diagnosis of inferior infarction does not necessarily identify
the artery branch that is occluded, unless you have a previous
coronary angiogram (an x-ray highlighting the coronary arteries)
to identify which
artery supplies the inferior portion
of that patient's left ventricle.
NOTE: Left or Right Coronary "dominance" denotes which coronary
artery is the major source of blood supply to the base of the left
ventricle. Right Coronary dominance is by far most common in humans.
|
Now
you know how to determine the specific arteries blocked in two important
types of infarction and which arteries are most likely to be blocked in
an inferior infarction. Pleased with your accomplishment?
|
|
Continue > >
|
|
|
Essential
Information for Physicians
Continue > >
|
|